
Cognitive Communication Disorder: Signs, Diagnosis, and Causes

A cognitive-communication disorder is a communication problem caused by changes in the thinking skills that support communication, including attention, memory, organization, processing speed, problem-solving, and self-monitoring.
Some adults with cognitive-communication disorders speak clearly and form sentences without difficulty, while others also have aphasia, dysarthria, apraxia, or voice changes. Communication breaks down because the person has trouble managing the cognitive demands of real-world conversation and daily interactions.
They may lose track of meetings, forget information that was just discussed, struggle to organize thoughts, miss social cues, repeat themselves, or have difficulty shifting topics appropriately.
Below, we explain what cognitive-communication disorders look like in adults, which cognitive domains are affected, how speech-language pathologists evaluate them, and how they may overlap with conditions like aphasia. The disorder often follows a neurological injury or condition such as traumatic brain injury, stroke, brain tumor, Parkinson’s disease, or dementia.
Key Takeaways
Cognitive-communication disorders affect a person’s ability to communicate effectively because of changes in cognitive skills such as attention, memory, executive functioning, processing speed, organization, social communication, and self-monitoring.
About 35 to 44 percent of stroke survivors experience cognitive impairment three months after a stroke, and a significant portion continue to have long-term difficulties, particularly after right hemisphere damage.
Diagnosis combines standardized testing with functional assessment by a speech-language pathologist, often after referral from a neurologist, rehabilitation physician, or other medical provider.
Common causes include traumatic brain injury, stroke, brain tumor, and progressive neurological conditions such as Parkinson’s disease, dementia, and multiple sclerosis. These conditions can affect the brain systems responsible for attention, memory, organization, and social communication.
What Is a Cognitive Communication Disorder?
How Cognitive Communication Disorders Present
What Cognitive Domains Are Affected
What Causes Cognitive Communication Disorders
How Cognitive Communication Disorders Are Diagnosed
Cognitive Communication Disorder vs. Aphasia
How Cognitive Communication Disorders Are Treated
What We See Working with Adults
Frequently Asked Questions About Cognitive Communication Disorder
How Connected Speech Pathology Can Help With Cognitive Communication Disorders
What Is a Cognitive Communication Disorder?

A cognitive communication disorder is a communication impairment caused by deficits in thinking. The condition is acquired, almost always linked to neurological injury or disease.
It may affect a person's ability to participate in conversations, follow directions, and manage everyday communication tasks. Some affected cognitive functions include attention, memory, executive function, organization, processing speed, reasoning, and awareness.
Adults with cognitive-communication disorders may speak fluently, but not always. Some also have aphasia, dysarthria, apraxia, or voice changes. The cognitive-communication breakdown often becomes more noticeable when the person has to follow a longer conversation, organize several ideas, respond quickly, remember details, or adjust to changing social demands.
The American Speech-Language-Hearing Association defines cognitive communication disorders as difficulties with any aspect of communication affected by a disruption in thinking. The field of speech-language pathology treats these disorders alongside aphasia and other related conditions because each person's profile of strengths and deficits is different.
How Cognitive Communication Disorders Present

Adults with cognitive-communication difficulties may speak clearly but still struggle with conversational organization, tracking details, maintaining attention, interpreting social cues, or keeping up with the flow of a discussion. The day-to-day presentation can look very different from a primary language disorder.
Someone with aphasia primarily has difficulty with language itself, while a person with cognitive-communication deficits may struggle more with the underlying cognitive processes that support communication, such as memory, attention, organization, self-monitoring, or executive functioning.
These cognitive-communication difficulties can affect both language use and the broader skills people rely on to communicate effectively in daily life, social situations, and the workplace.
Common signs and symptoms in adults include:
Difficulty following multi-step directions or instructions delivered quickly
Losing track of the topic mid-conversation or going off on tangents
Memory problems for recent conversations, names, or details that surface soon after they happen
Difficulty concentrating in fast-paced or busy environments
Attention problems that show up when the cognitive load rises
Missing visual cues from a speaker, including facial expressions and gestures
Trouble reading nonverbal cues during conversation, including tone shifts and sarcasm
Word-finding difficulties that surface under cognitive load
Difficulty with reading and writing for tasks that used to feel automatic
Frustration and anxiety during conversations that previously felt easy
Trouble filtering background noise during meetings or group settings
Cognitive-communication deficits can affect daily life in many different ways. Conversations, reading, writing, multitasking, and group discussions may become more effortful or overwhelming, particularly in busy or demanding environments. Some individuals notice changes in memory, reasoning, judgment, attention, or social communication that make it harder to follow conversations and shared experiences.
Depending on the severity and underlying cause, these communication difficulties may also affect workplace performance, relationships, and everyday responsibilities like managing schedules, medications, or finances. In some cases, communication changes are among the first symptoms families notice before the underlying cognitive condition has been fully identified.
What Cognitive Domains Are Affected
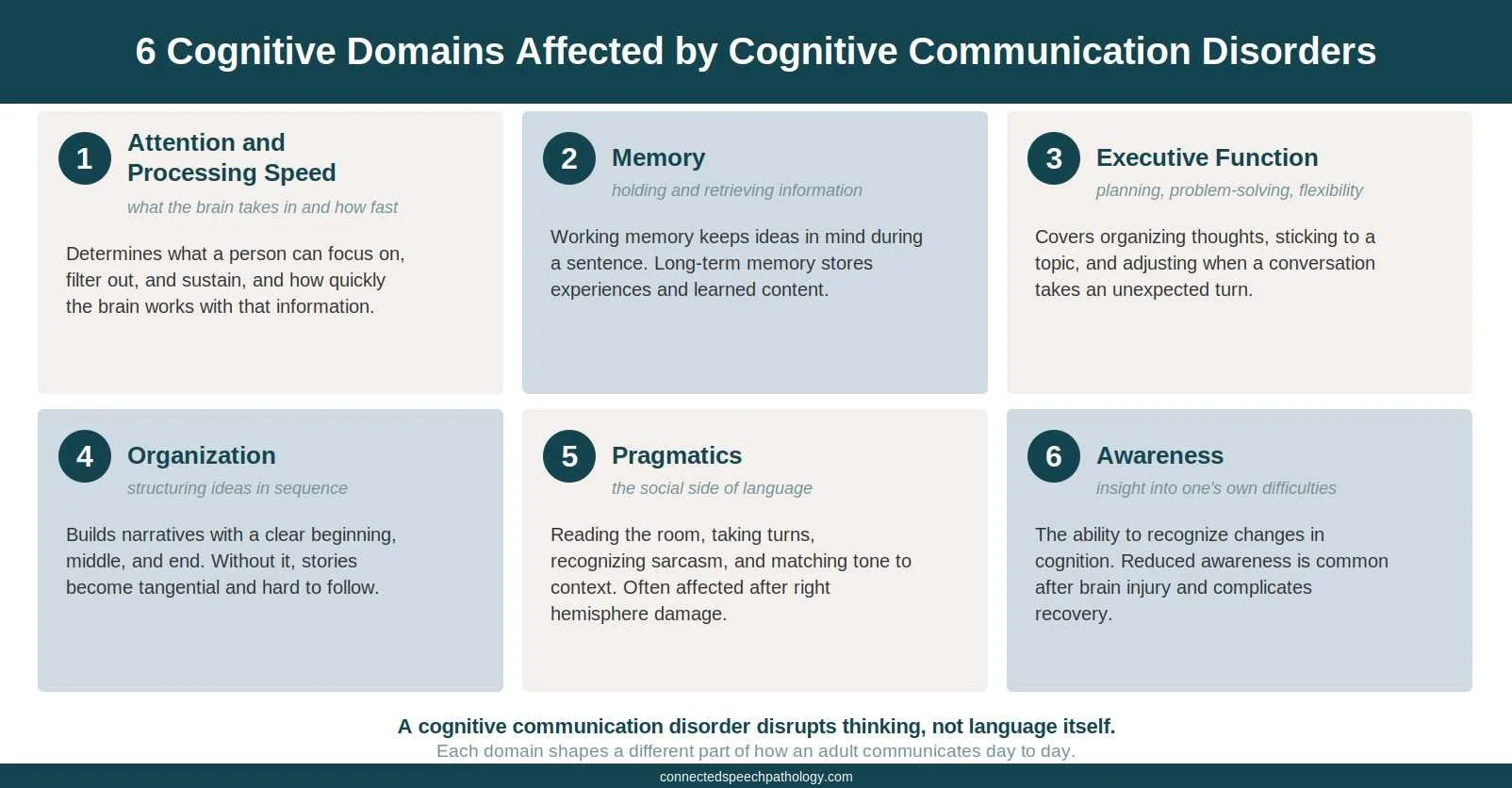
Each domain shapes a different aspect of how an adult communicates. The six most commonly affected are attention and processing speed, memory, executive function, organization, pragmatics, and awareness. A breakdown in any one of them can lead to noticeable changes in conversation, problem-solving, and daily interactions.
Attention and Processing Speed
Attention determines what a person can focus on, filter out, and sustain. Processing speed determines how quickly the brain takes in and works with that information.
When either slips, conversations move faster than the listener can track, and instructions slip past before they are fully absorbed.
Memory
Working memory holds information in mind long enough to use it, like keeping the start of a sentence in mind while finishing it. Long-term recall stores experiences and learned information.
For more on this domain specifically, see our guide to speech therapy for memory loss.
Adults with this difficulty often forget what was just said, what they intended to say, or what was discussed earlier in the same conversation. The difficulty compounds in longer or more demanding situations.
Executive Function
Executive function encompasses planning, organizing, problem-solving, and flexibly shifting between tasks. A breakdown shows up as trouble organizing thoughts before speaking, sticking to a topic, or adjusting when a conversation takes an unexpected turn.
Problem-solving slows in real time, and the everyday tasks that depend on it, like sequencing project steps, become harder to manage.
Organization
Organization in communication means structuring ideas in a logical sequence, like telling a story with a clear beginning, middle, and end, or explaining a process in steps. Without it, narratives may become tangential, and listeners struggle to follow.
Pragmatic Language
Pragmatic language is the social side of communication: reading the room, taking conversational turns, recognizing sarcasm or indirect meaning, and adjusting language to fit the situation. Pragmatic difficulties are common after right hemisphere damage, traumatic brain injury, and other neurological conditions, even when basic language skills appear relatively intact.
Some specialists describe these patterns as right hemisphere communication disorders or social communication impairments. In these cases, speech may sound fluent on the surface, but the timing, relevance, organization, or social interpretation of the conversation may be affected.
Awareness
Awareness, or insight, is the ability to recognize one's own difficulties. Reduced awareness is common after brain injury and complicates recovery, because an adult who does not recognize the changes resists strategies that would help.
What Causes Cognitive Communication Disorders
Cognitive-communication disorders are most commonly associated with neurological injury, disease, or other conditions that affect brain functioning. They can involve disruptions in attention, memory, executive functioning, processing speed, organization, and problem-solving, and often overlap with language disorders such as aphasia or motor speech disorders.
The presentation varies depending on the underlying cause, the areas of the brain affected, and the severity of the impairment, which is part of why diagnosis and treatment planning require a trained clinical perspective.
Right hemisphere stroke often produces a fluent, grammatically intact speaker who wanders off topic, misses sarcasm, and loses the social timing of a conversation.
Left hemisphere stroke can produce aphasia and cognitive communication deficits at the same time. Differential diagnosis matters here because the right plan depends on which deficit pattern is driving the breakdown.
Traumatic brain injury (TBI) typically hits executive function and attention first, even in mild cases. The early signs are subtle: slower processing in meetings, a harder time tracking multi-step instructions, and fatigue that compounds across the day. See the complete guide to TBI speech therapy for clinical specifics.
Brain tumor symptoms depend on location and rate of growth. Slow-growing tumors can produce gradual personality and attention changes that families attribute to stress or aging until imaging confirms the cause.
Dementia, including Alzheimer's disease, follows a progression. Word-finding difficulty and short-term memory loss appear first, organization and reasoning follow, and pragmatic deficits often emerge later in the course.
Parkinson's disease and other movement disorders affect processing speed and word retrieval before they affect general cognition. Adults often describe knowing what they want to say but losing access to it under time pressure.
Multiple sclerosis produces cognitive changes alongside motor symptoms, often in attention and processing speed. The fluctuating course makes the timing of assessment important.
Anoxic or hypoxic brain injury from cardiac arrest, near-drowning, or other oxygen disruption can produce diffuse cognitive deficits. Some long-term effects also appear after viral illness, including post-COVID cognitive decline.
Approximately 35 to 44 percent of stroke survivors experience cognitive impairments three months after the event. About one-third face long-term cognitive issues, particularly after right hemisphere strokes.
Although cognitive-communication disorders are most commonly associated with neurological conditions, cognitive-communication symptoms can also be worsened by factors such as medication side effects, severe fatigue, metabolic illness, or other medical conditions that affect cognitive functioning.
Cognitive impairment is a common consequence of brain injury, and the risk is high and often underrecognized because the symptoms can be subtler than the motor or language symptoms that families expect to see.
How Cognitive Communication Disorders Are Diagnosed

Diagnosis starts with a referral. Neurologists, primary care physicians, and rehabilitation teams typically refer a patient after a brain injury, stroke, or progressive disease.
A speech-language pathologist conducts a comprehensive evaluation to identify which cognitive and communication processes are affected and how those difficulties appear in real-world situations. Assessment also helps clarify whether the primary breakdown involves cognitive-communication, language, motor speech, or a combination of factors, so treatment can be tailored appropriately.
Cognitive communication disorders can be identified using the Cognitive-Communication Checklist for Acquired Brain Injury (CCCABI), a free online screening tool. The CCCABI helps lead speech-language pathologists to adults who would benefit from a full assessment.
Assessment for cognitive communication disorders typically includes both formal and informal tools. Formal measures include standardized tests, such as the Arizona Battery for Cognitive Communication Disorders or the Behavior Rating Inventory of Executive Function.
Informal tools cover conversation samples, structured interviews, and patient-reported outcome measures. Together, they let speech-language pathologists create personalized care plans based on the patient's functional needs.
A thorough evaluation covers several areas:
Attention and processing speed under varying cognitive load
Working memory and longer-term recall
Executive function tasks, including planning and problem-solving
Language skills, comprehension, and expression to rule out a primary language disorder
Pragmatics in structured social tasks
Reading and writing skills
Self-awareness of difficulties
The speech-language pathologist also gathers history from family members or caregivers, because awareness deficits often lead adults to under-report their own changes. The combined picture produces a diagnosis and a roadmap for care.
Cognitive Communication Disorder vs. Aphasia

The distinction matters. The two conditions look similar on the surface but respond differently to speech therapy approaches.
Aphasia is primarily a language disorder. Damage to the brain's language centers, usually in the left hemisphere, disrupts the ability to find words, produce grammatical sentences, understand speech, or read and write.
Speech can be halting, telegraphic, or filled with paraphasias. The cognitive systems around it often remain intact.
In some people with cognitive-communication disorder, basic language structure remains relatively intact, with sentences and grammar appearing largely preserved, while the cognitive processes that support communication begin to break down.
An adult with a right hemisphere stroke may produce fluent, grammatically correct speech while still struggling with topic maintenance, conversational organization, social cues, or interpreting the context of a discussion.
The two can co-occur. A left hemisphere stroke that causes aphasia can also produce cognitive deficits.
Differential diagnosis requires careful testing of both language and cognition. Speech therapy for aphasia differs from speech therapy for cognitive communication disorder. See the related guide to aphasia vs. apraxia for another related comparison.
How Cognitive Communication Disorders Are Treated

Care is functional and individualized. Plans include compensatory strategies, environmental modifications, and speech and language therapy techniques.
Treatment strategies are delivered by a speech-language pathologist, often in coordination with neurologists, occupational therapists, and physical therapists. The plan reflects each person's ability, goals, and daily demands.
Assistive technology may include augmentative and alternative communication (AAC) devices, text-to-speech applications, and other tools that support communication and expression. Family training is essential. It teaches practical communication strategies and helps establish supportive environments that make the cognitive load manageable.
For a full walkthrough of clinical approaches, evidence-based protocols, and what cognitive speech therapy sessions look like, see the complete guide below.

Cognitive Speech Therapy for Adults
Check out our blog on cognitive speech therapy for adults for more information!
What We See Working with Adults
Two patterns commonly arise in our work with cognitive-communication deficits. Some adults come to speech therapy after a brain injury or stroke, while others begin noticing gradual cognitive and communication changes over time.
One mid-career professional returned to work after a mild traumatic brain injury and found that meetings became mentally exhausting in a way they had never been before. She could follow individual comments but had difficulty keeping track of longer discussions, shifting topics, and the fast-paced social demands of leadership meetings.
By the second half of the day, she often realized she had stopped fully processing the conversation. Speech therapy focused on attention strategies, structured note-taking, pacing techniques, and real-world communication supports designed around her work environment. Within a few months, she was able to get through full meeting days with better carryover, improved organization, and notes she could reliably use afterward.
Another client came to speech therapy after a right hemisphere stroke. His wife noticed subtle changes first: stories became harder to follow, conversations drifted off topic, and he missed cues that once helped him navigate everyday social interactions.
His speech still sounded fluent, which made the changes more difficult for family members and coworkers to recognize. Speech therapy focused on pragmatic language, conversational organization, self-monitoring, and structured social communication practice to help rebuild the skills his daily interactions depended on.
Frequently Asked Questions About Cognitive Communication Disorder
1. What is the difference between a cognitive communication disorder and aphasia?
Aphasia primarily affects the language system itself, including speaking, understanding, reading, and writing. Cognitive-communication disorders primarily affect the cognitive processes that support communication, such as attention, memory, organization, processing speed, and executive functioning, although some individuals may experience overlap between the two.
2. Can cognitive communication disorders be cured?
There is no cure, but improvement is possible. Recovery depends on the cause, the severity, and how early speech therapy begins. Speech-language pathologists focus on restoring function where possible and teaching compensatory strategies for the deficits that remain.
3. Who diagnoses a cognitive communication disorder?
A speech-language pathologist makes the diagnosis in cooperation with the treating medical physician. Referral usually comes from a neurologist, primary care physician, or rehabilitation team. Diagnosis combines standardized testing with functional assessment.
4. How long does speech therapy for a cognitive communication disorder last?
Length varies based on the cause and severity. Acute stroke or TBI recovery often involves weeks to months of regular sessions. Progressive conditions like dementia or Parkinson's disease benefit from ongoing intermittent support to adjust strategies as the disease changes.
5. Can a cognitive communication disorder develop without a clear brain injury?
Yes, in progressive neurological disease. Conditions like Alzheimer's, primary progressive aphasia, and Parkinson's produce a gradual cognitive decline rather than a single injury event. The disorder unfolds over time rather than appearing suddenly.
How Connected Speech Pathology Can Help With Cognitive Communication Disorders

Connected Speech Pathology supports adults living with cognitive communication deficits after stroke, traumatic brain injury, brain tumor, and progressive neurological conditions.
Our speech-language pathologists conduct a comprehensive evaluation, identify the affected cognitive functions, and develop a plan built around your real-life communication and social communication demands. Each person we work with has a different cognitive profile, so the plan reflects how the disorder affects their daily life, work, and relationships.
Every session takes place online, eliminating the difficulty of travel during a period when fatigue and cognitive load are already taxing. Sessions are scheduled around your routines, and family members can join when training is part of the plan.
Summary
A cognitive communication disorder is a communication impairment caused by deficits in attention, memory, executive function, organization, processing speed, pragmatics, or awareness. It is not damage to the language or speech systems themselves.
Cognitive communication deficits are acquired, almost always tied to a neurological event or condition like stroke, traumatic brain injury, brain tumor, Alzheimer's disease, or Parkinson's disease. Diagnosis sits within the field of speech-language pathology and requires both standardized assessment tools and functional evaluation. Speech therapy focuses on restoring cognitive function where possible and building compensatory strategies for the cognitive communication deficits that remain.
If you suspect a cognitive communication disorder, a speech-language pathology assessment is the right next step.

About the Author
Allison Geller, M.A., CCC-SLP, is a communication coach, speech-language pathologist, and founder of Connected Speech Pathology, an international online practice providing professional communication coaching and speech therapy for children, teens, and adults. With more than two decades of experience, she has worked in medical and educational settings and published research on aphasia. Today, she leads a team of specialists who help clients improve their skills in public speaking, vocal presence, accent clarity, articulation, language, fluency, and interpersonal communication.