
Cognitive Speech Therapy for Adults: A Guide to Evidence-Based Treatment

A stroke, brain injury, or memory condition rarely affects just one piece of communication. Word-finding, attention, conversation tracking, and clear thinking often go together, and the resulting communication difficulties show up as both difficulty speaking and difficulty following what others are saying.
Cognitive speech therapy targets that gap directly. It is the branch of speech-language pathology that treats the thinking skills behind communication: attention, memory, word retrieval, and executive function. Adults with cognitive impairments after a stroke, brain injuries, Alzheimer's disease, mild cognitive impairment, or post-COVID cognitive decline often benefit from cognitive speech therapy.
Read on for what cognitive speech therapy is, who it helps, the evidence-based techniques speech-language pathologists use, and what to expect from sessions. We also cover at-home practice and answer common questions about coverage and online delivery.
Key Takeaways
Cognitive speech therapy treats the thinking skills behind communication. A speech-language pathologist targets attention, memory, word retrieval, and executive function when those skills affect how an adult talks, listens, or follows conversation.
It serves adults with neurological causes. Stroke, brain injuries, dementia, Alzheimer's disease, mild cognitive impairment, post-COVID cognitive decline, and Parkinson's disease are common reasons adults start cognitive speech therapy for communication challenges.
Techniques can be evidence-based and specific, but progress is not driven by protocols alone. Spaced retrieval, Semantic Feature Analysis, Response Elaboration Training, and metacognitive strategy training all have research support. The INCOG guidelines from Jennie Ponsford and colleagues are a current standard for adults after traumatic brain injury. Treatment also depends on the person's goals, environment, insight, fatigue levels, and daily communication demands.
Progress comes from functional practice tied to real situations. Apps and software-based memory drills can support independent practice between sessions. Daily exercises connected to real conversations, routines, and tasks are more likely to carry over into everyday communication.
What Is Cognitive Speech Therapy?
Who Cognitive Speech Therapy Helps
What Areas Does Cognitive Speech Therapy Target?
Evidence-Based Techniques Used in Cognitive Speech Therapy
What Cognitive Speech Therapy Sessions Look Like
What We See Working With Clients
Frequently Asked Questions About Cognitive Speech Therapy
How Connected Speech Pathology Can Help With Cognitive Speech Therapy
What Is Cognitive Speech Therapy?

Cognitive speech therapy is a type of treatment for adults delivered by a speech-language pathologist. It targets the cognitive processes that affect communication: attention, memory, word retrieval, problem-solving, and executive function. The goal is functional improvement in daily conversation and decision-making for adults with neurological causes, including stroke, brain injuries, or dementia.
You will also see this work referred to as cognitive-communication therapy or cognitive rehabilitation. Terminology shifts by setting, with acute care often using "cognitive rehabilitation" and outpatient communication services leaning toward "cognitive speech therapy." Speech-language pathologists play a critical role in assessing and treating the cognitive deficits that affect daily living, often through interdisciplinary collaboration with neurologists, physical therapists, and occupational therapists.
What sets cognitive speech therapy apart from other types of speech therapy is its focus. Articulation therapy and voice therapy address how sounds and the voice are produced. Cognitive speech therapy addresses the mental processes that organize thoughts into words and the cognitive abilities that hold a conversation together.
Who Cognitive Speech Therapy Helps

Cognitive speech therapy serves adults whose thinking skills have been affected by a neurological event or disease. Cognitive speech therapy can be effective at any age. Common causes include:
A stroke that disrupts blood flow to areas of the brain involved in attention, language skills, or memory.
Traumatic brain injury from falls, vehicle accidents, or sports. Our TBI speech therapy guide covers brain injuries and recovery in depth.
Alzheimer's disease and other forms of dementia, where memory loss and word-finding difficulty are early signs.
Mild cognitive impairment that affects memory or focus without meeting criteria for dementia, sometimes called mild impairment in the early stages.
Post-COVID cognitive decline, sometimes called brain fog, affects attention, word retrieval, and verbal expression.
Parkinson's disease and related conditions that bring cognitive changes alongside motor symptoms, often including communication challenges that benefit from voice therapy.
Brain tumors, brain infections, anoxic brain injuries, and other neurological conditions that disrupt cognitive and language functioning.
Primary progressive aphasia and other neurodegenerative conditions affecting language and cognitive skills.
Older adults with these diagnoses commonly notice the same patterns. Losing focus mid-conversation, word-finding pauses, difficulty following long instructions, and trouble organizing thoughts before speaking. These are cognitive communication impairments, sometimes called cognitive communication deficits, and they respond to targeted speech therapy.

Cognitive Communication Disorder
Check out our blog on cognitive communication disorder for more information!
What Areas Does Cognitive Speech Therapy Target?
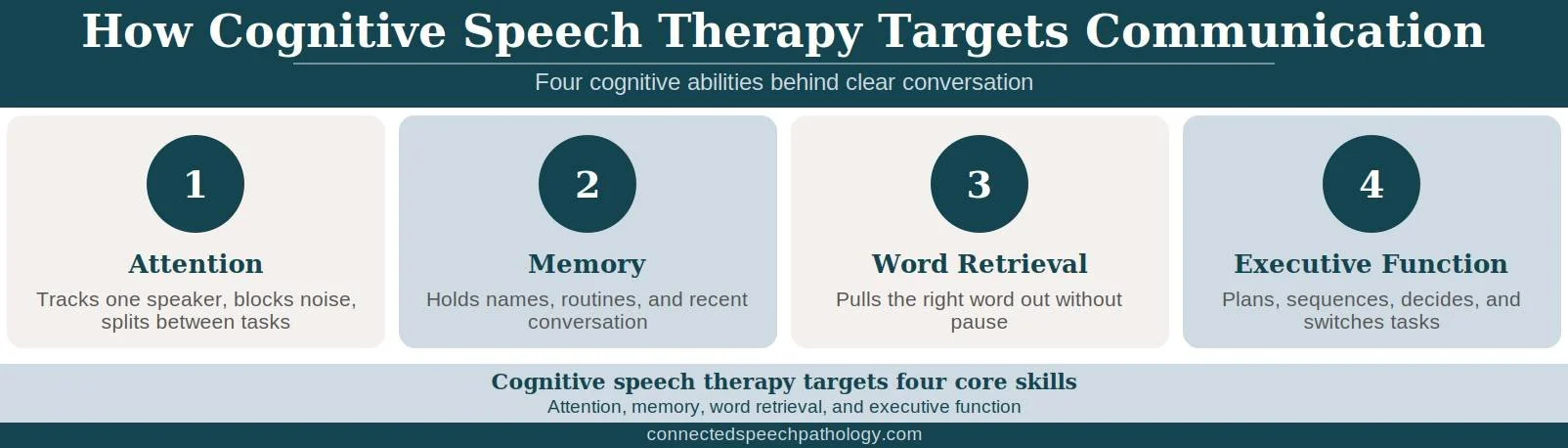
A speech-language pathologist focuses cognitive speech therapy on four core cognitive abilities that shape communication. Each area has its own assessment tools and intervention approaches, and matching the right strategies and visual aids to the deficit pattern is what separates effective cognitive rehabilitation from generic brain training.
Attention
Attention controls what you notice, hold, and act on during a conversation. Sustained attention keeps you tracking a single speaker, selective attention filters out background noise, and divided attention lets you listen and take notes at once. Maintaining focus across these channels is the first target of cognitive speech therapy after brain injuries.
The INCOG attention guidelines from Ponsford and colleagues recommend screening for sleep, pain, vision, fatigue, and medication effects before beginning any attention work. Patient education on those triggers is part of the protocol. Attention exercises later on include practicing conversations while ignoring distractions or transitioning between tasks under controlled timing.
Memory
Memory difficulties show up as forgetting recent conversations, repeating questions, missing appointments, or struggling to recall familiar names. Speech therapy in this area targets short-term recall, working memory used during conversation, and the procedural knowledge needed for daily routines. Memory loss after stroke or dementia responds well to evidence-based memory strategies and external aids when matched to the right severity of cognitive deficits.
Word Retrieval and Language
Word-finding difficulty is one of the most common reasons adults seek cognitive speech therapy and a defining feature of aphasia after stroke. The right words feel just out of reach when you try to express thoughts mid-sentence, and the workaround sentences that follow can sound less precise than intended, which, over time, can pull adults back from social interactions. Cognitive speech therapy uses language retraining and cueing techniques to rebuild verbal expression, and gains in cognitive function tend to lift communication skills alongside word access.
Executive Function
Executive functions include planning, sequencing, problem-solving, and decision-making. They are what let you organize a story before telling it, track your point through a long answer, and shift smoothly between tasks in daily life.
When executive function is impaired, communication becomes harder to organize and easier to derail, and the cognitive challenges spill into everything from grocery shopping to running a meeting. Cognitive speech therapy targets these abilities through structured practice tied to real daily demands.
Evidence-Based Techniques Used in Cognitive Speech Therapy
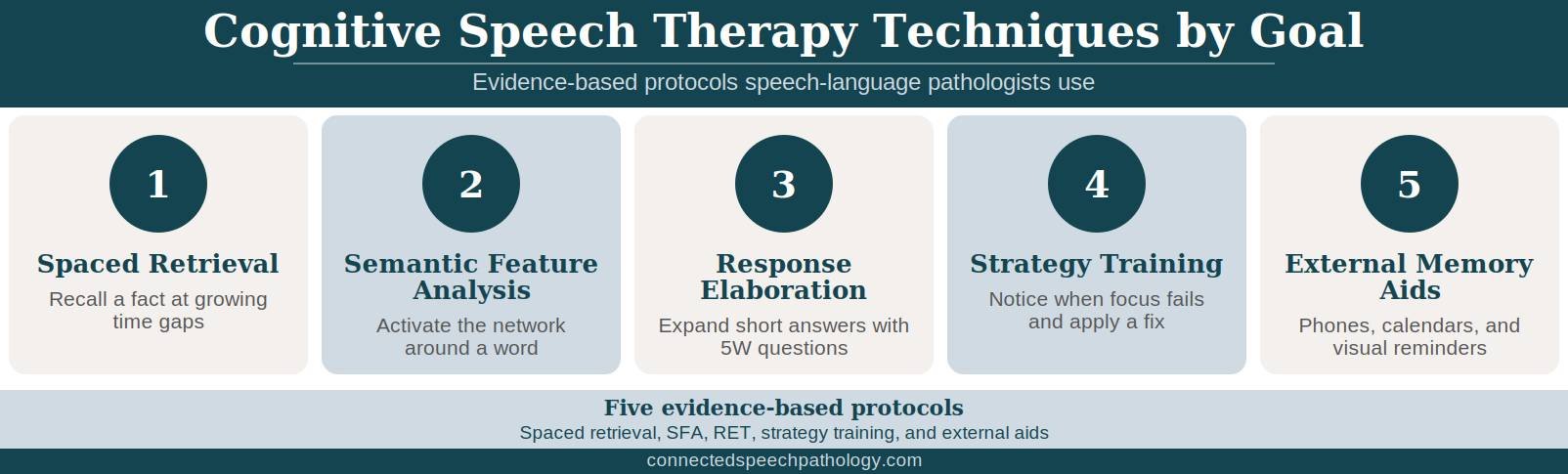
The protocols below are the methods speech-language pathologists draw on most often. Each one has research support behind it and targets specific cognitive abilities rather than general brain training.
Spaced Retrieval
Spaced retrieval is a memory training technique that asks the patient to recall a target fact at progressively longer intervals, starting at a few seconds and extending outward. Facts recalled successfully stick, and those that miss are reviewed and re-cued before the next attempt. The protocol is particularly useful for learning names, daily routines, or safety information in patients with dementia or traumatic brain injury.
Semantic Feature Analysis
Semantic Feature Analysis stimulates word retrieval through structured grids. The patient generates information about a target word across categories like group, function, location, and physical features. Each grid activates the semantic network around the target and helps the right word surface more reliably during conversation, and the protocol is one of the most studied options for word-finding difficulty after stroke.
Response Elaboration Training
Response Elaboration Training, or RET, builds longer and more informative spoken responses. The speech-language pathologist presents an image of an action and asks 5W questions, meaning who, what, when, where, and why, to expand the patient's initial response. There are no correct answers, which is why RET is sometimes called "loose training," and the technique helps adults who can produce single words but struggle to form complete thoughts in conversation.
Metacognitive Strategy Training
Metacognitive strategy training teaches patients to recognize when their attention or executive function is failing and apply a specific strategy in response. INCOG lists this approach as Level A evidence for mild-to-moderate attention deficits after traumatic brain injury, the highest evidence rating the guidelines assign. The strategies are tied to functional everyday activities rather than computer drills, which the same guidelines note do not reliably transfer to real life.
External Memory Aids
Phones, notebooks, whiteboards, alarms, visual aids on the fridge, and shared family calendars compensate for memory impairments that are slow to resolve or unlikely to. Visual aids placed in the patient's environment can prompt memory recall throughout the day without depending on internal cues. INCOG recommends external supports, especially for adults with severe memory impairment, and training both the patient and a family member in how to use the tools consistently is part of the protocol.
What Cognitive Speech Therapy Sessions Look Like

A first cognitive speech therapy visit usually starts with an assessment. A speech-language pathologist reviews medical history, talks with the patient and a family member about daily communication problems, and runs cognitive and language tasks to pinpoint the most affected areas. Interdisciplinary collaboration with the patient's neurologist or primary care provider often improves outcomes.
Standardized tests are sometimes part of this, though functional observation of conversation, problem-solving, and recall often provides the most useful information. Speech-language pathologists frequently observe shared patterns across neurological conditions rather than applying a unique test battery for each diagnosis.
The cognitive speech therapy plan is based on that assessment. A return-to-work goal looks different from a regain-control goal at home, and the techniques used reflect what success and increased independence mean for that adult. Sessions then alternate between practicing the chosen techniques and applying them to real situations the patient brings in.
Cognitive speech therapy can be delivered in person or through telehealth. Online delivery is now part of mainstream cognitive rehabilitation, and the INCOG update included new recommendations supporting telehealth-delivered cognitive assessment and cognitive rehabilitation. For adults recovering at home, remote sessions can sometimes be more convenient than driving to an outpatient clinic.
Communication Partner Training
Cognitive communication therapy works better when the people the patient talks to every day are trained too. Partner training is central to improving communication skills and well-being among adults with cognitive deficits, since most conversations occur outside the session. The speech-language pathologist coaches a family member or close colleague on how to slow down, simplify questions, and use visual aids that support verbal expression.
Barriers to partner training include lack of availability, time, and receptiveness among those closest to the patient. When those barriers are present, the cognitive speech therapy plan should still include a written communication plan for a consistent approach. Social pragmatic interventions, including role-playing and non-verbal cue training, also help adults use language contextually in interpersonal relationships.
At-Home Practice Between Sessions
Practice between sessions speeds progress more than session frequency does. Useful at-home activities include:
Calendar tasks like writing tomorrow's plan and reviewing yesterday's appointments.
Daily journaling, even a few sentences, to practice organized written expression.
Word-finding games, such as categories, where you name ten kitchen items in a minute, and 20 questions.
Recipe sequencing or following written instructions to rebuild planning and comprehension. These tasks also strengthen reading comprehension, a common goal for adults in cognitive speech therapy.
Conversation practice with a family member focused on a specific goal, like staying on topic.
Apps can support cognitive speech therapy when they target the right skill. Spaced retrieval programs from Tactus and structured drill platforms like Constant can extend practice between sessions. These tools work best paired with a speech-language pathologist who can match drills to the patient's goals and review progress.
What We See Working With Clients

A few patterns often come up in our cognitive speech therapy practice that are worth sharing. Both scenarios below show how targeted protocols assist individuals with distinct cognitive impairments and distinct goals.
One client returned to a management role at a large logistics company after a traumatic brain injury from an automobile accident. Casual conversation sounded mostly normal, but work conversations broke down under pressure. He lost track of multi-step discussions in meetings, struggled to retrieve specific business terms during presentations, and forgot action items unless they were written down immediately.
We focused on metacognitive strategy training tied to his actual workday. Sessions used his meeting agendas, project updates, and email drafts rather than generic exercises. We also worked on self-cueing for word retrieval, note organization, and strategies for tracking multiple speakers during fast conversations. After several months, he was leading shorter team meetings again and relying less on coworkers to fill in gaps when he lost a word or train of thought.
Another client came in with early memory difficulties after a prolonged COVID-19 illness, a pattern we cover separately in our post-COVID cognitive decline guide. She was missing appointments, repeating questions to her husband, and frustrated that conversations from a few days earlier had vanished, which pulled her back from the social interactions she used to enjoy.
We set up a phone-based external memory aid system with linked calendar reminders and a shared notes app, then trained spaced retrieval for the names and routines that mattered most to her week. Six weeks in, her husband reported far fewer repeat questions, reliable recall of daily appointments, and that she was running her own schedule again with increased independence, needing only light prompts.
Frequently Asked Questions About Cognitive Speech Therapy

1. How long does cognitive speech therapy take to show results?
Most adults notice a change in 6 to 12 weeks of weekly sessions. Recovery from stroke or traumatic brain injury continues for months and often years, and the rate of progress depends on injury severity, time since onset, any significant past medical history, and how much functional practice happens between sessions.
2. Can cognitive speech therapy be done online?
Yes. Cognitive speech therapy is well-suited to telehealth, and the INCOG guidelines now include recommendations for telehealth-delivered cognitive rehabilitation. Online sessions use the same assessments and protocols as in-person speech therapy, with the added benefit that practice happens in the patient's actual home environment.
3. What's the difference between cognitive speech therapy and traditional speech therapy?
Traditional speech therapy often means speech articulation, voice, or fluency work. Cognitive speech therapy addresses the thinking skills behind communication: attention, memory, word retrieval, and executive function. Many adults need both after a stroke or brain injury, and a single speech-language pathologist usually delivers both.
4. Does insurance cover cognitive speech therapy?
Coverage depends on the diagnosis, the plan, and the setting. Connected Speech Pathology is a private-pay practice and does not bill insurance directly. Many clients use HSA or FSA funds to cover sessions, and some employer-paid professional development funds apply when communication impacts work.
5. Can cognitive speech therapy help with dementia?
Yes, with realistic goals. Cognitive speech therapy cannot reverse Alzheimer's disease or other dementias, but a cognitive speech therapy program can preserve communication function longer, set up external memory aids, and train family members to support conversation. The focus shifts from improving communication skills to maintaining them, which still matters for the patient's well-being as cognitive impairments progress.
How Connected Speech Pathology Can Help With Cognitive Speech Therapy

Connected Speech Pathology offers cognitive speech therapy for adults through online sessions. Our speech-language pathologists assess the specific cognitive abilities that affect your communication, then build a plan around the goals that matter in your life, whether that is returning to work, running a household, or staying engaged with family.
Sessions combine the evidence-based protocols described earlier with practice in your real environment. Family members can join sessions to learn strategies that research shows improve outcomes and well-being for adults with cognitive-communication impairments.
If you are an adult recovering from a stroke, traumatic brain injury, or living with a memory condition, our speech-language pathologists can help you rebuild the cognitive skills behind communication. Your first call is a free consultation to talk through your situation and decide together whether cognitive speech therapy is the right next step.
Summary
Cognitive speech therapy is the branch of speech-language pathology that treats the thinking skills behind communication for adults with stroke, brain injuries, Alzheimer's disease, and other neurological causes. Speech-language pathologists use evidence-based techniques such as spaced retrieval, Semantic Feature Analysis, Response Elaboration Training, and metacognitive strategy training to target cognitive deficits that affect daily life, with the INCOG guidelines from Bayley and Ponsford as the current standard for traumatic brain injury.
Functional practice tied to your daily life beats generic brain training, and online delivery makes this care accessible from home.

About the Author
Allison Geller, M.A., CCC-SLP, is a communication coach, speech-language pathologist, and founder of Connected Speech Pathology, an international online practice providing professional communication coaching and speech therapy for children, teens, and adults. With more than two decades of experience, she has worked in medical and educational settings and published research on aphasia. Today, she leads a team of specialists who help clients improve their skills in public speaking, vocal presence, accent clarity, articulation, language, fluency, and interpersonal communication.