
Aphasia vs. Apraxia: What Is the Difference?
Aphasia and apraxia of speech share so many surface symptoms that even seasoned speech-language pathologists take time to tell them apart. Both can follow a stroke. Both can leave an adult struggling to say the right word.
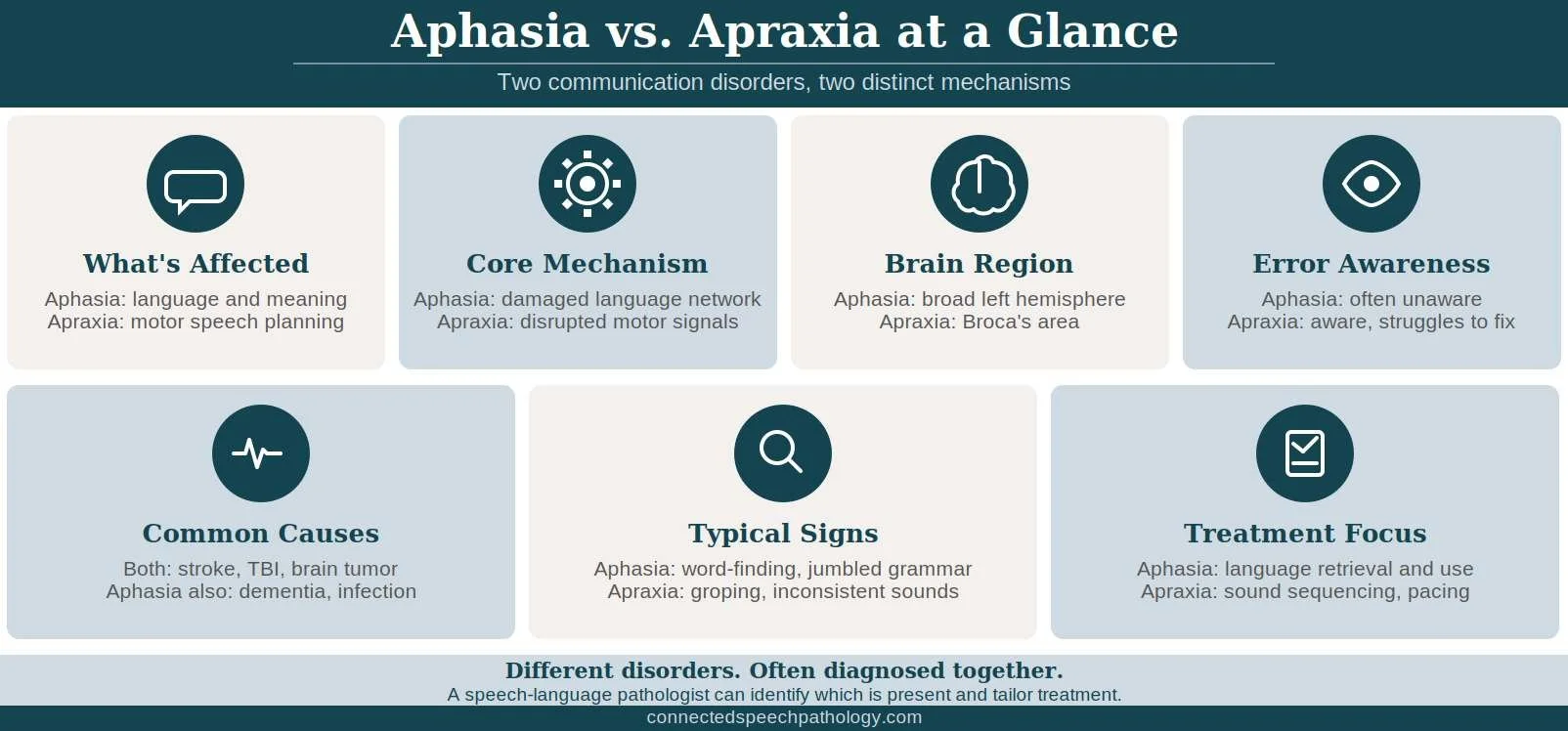
The difference comes down to what’s going wrong in the brain, and it changes everything about treatment. Aphasia is a language disorder that disrupts how the brain processes meaning, while apraxia of speech is a motor planning disorder that disrupts how the brain coordinates the muscles used for speaking.
What follows breaks down the distinct mechanisms, signs, and treatment approaches behind each condition. You will see how the two often co-occur, how a speech-language pathologist distinguishes between them, and what daily support looks like for an adult living with either disorder.
Key Takeaways
Aphasia is a language disorder; apraxia of speech is a motor planning disorder. Aphasia disrupts how the brain processes words and meaning, while apraxia disrupts how the brain coordinates the mouth, lips, and tongue movements needed to produce sounds.
Both conditions usually result from damage to the left hemisphere of the brain. Stroke and traumatic brain injuries are the leading causes for adults, with tumors and neurodegenerative diseases also implicated.
The two disorders frequently occur together. Many adults with apraxia of speech also have some degree of aphasia, since the brain regions that handle language and motor speech planning sit close to one another.
Speech-language pathologists treat both conditions, and treatment is built around each adult's specific symptom profile. Therapy targets language retrieval and use for aphasia, and sound sequencing and motor planning for apraxia, with both approaches often running in parallel.
What's the Difference Between Aphasia and Apraxia?
What Causes Aphasia and Apraxia?
How Aphasia and Apraxia Are Diagnosed
How to Support Someone With Aphasia or Apraxia
What We See Working With Clients
What Is Aphasia?

Aphasia is a language disorder caused by damage to the brain's language network, most often in the left hemisphere. It affects the ability to use and understand words across speaking, listening, reading, and writing.
An adult with aphasia knows what they want to say but cannot reliably retrieve, sequence, or comprehend language. Some people lose access to specific words; others speak fluently but produce sentences that lack meaning. The pattern depends on which language regions sustained damage, which our guide to aphasia and its types covers in depth.
Common Symptoms of Aphasia
Symptoms vary in severity, and a single person rarely shows all of them. Most adults with aphasia experience a combination of the following challenges:
Trouble finding words. A familiar object, name, or place becomes inaccessible mid-sentence, sometimes called a tip-of-the-tongue feeling that does not resolve.
Speaking in fragments or jumbled sentences. Grammar breaks down, function words drop out, or fluent speech flows without meaning.
Difficulty understanding others. Spoken language and written text can become hard to follow, especially when the pace is fast or the topic shifts.
Reading and writing struggles. The same processing breakdown affects all language modalities, not just speaking.
Trouble with numbers. Counting, simple arithmetic, and managing finances often become harder, since numbers rely on the same language systems.
What Is Apraxia of Speech?

Apraxia of speech is a motor planning disorder. The brain knows what it wants to say, and the muscles are physically capable of moving, but the signal that tells those muscles how to coordinate gets disrupted.
An adult with apraxia of speech often produces distorted, inconsistent sounds and visibly struggles to position the lips, tongue, and jaw. Unlike aphasia, language comprehension stays largely intact, and the person usually knows their speech is coming out wrong. Awareness without the ability to self-correct is one of the most frustrating aspects of the condition, particularly when it overlaps with an articulation disorder.
Common Symptoms of Apraxia
Apraxia of speech presents through patterns that distinguish it from other motor speech and language disorders. Look for the following signs:
Inconsistent speech errors. The same word can come out correctly one moment and incorrectly the next, even within the same conversation.
Visible groping movements. Many adults reposition the tongue, lips, or jaw mid-word, searching for the correct articulatory placement.
Slow, effortful speech. Sound transitions feel labored, and longer phrases collapse more often than short ones.
Awareness of mistakes. The person hears the error and tries to self-correct, but repeated attempts do not always improve clarity.
Difficulty with rhythm and stress. Prosody flattens or sounds robotic because it also depends on motor coordination.
The flatness or inconsistency in rhythm is one reason adults with apraxia sometimes describe their voice as sounding like it belongs to someone else, and targeted work on prosody of speech can help restore some of the natural cadence.
What's the Difference Between Aphasia and Apraxia?
Aphasia is a language disorder that affects how the brain processes meaning, while apraxia of speech is a motor planning disorder that affects how the brain coordinates the muscles used for speaking. Aphasia disrupts language itself; apraxia disrupts the physical execution of speech. Both can result from the same underlying neurological injury, which is why they often appear together.
The clearest way to picture the difference is to think about where the breakdown happens in the chain from thought to spoken word. Aphasia interferes with finding and assembling the words; apraxia interferes with executing the mouth movements once the words are ready to come out.
An adult with pure aphasia can produce fluent speech that lacks meaning or struggle to retrieve a familiar name despite having intact articulation. An adult with pure apraxia knows exactly what they want to say but cannot get the sounds to come out correctly, while their reading, writing, and comprehension stay intact.
In practice, the two rarely appear in pure form after a stroke or brain injury. The brain regions responsible for language and motor speech planning sit close together in the left hemisphere, so a single lesion often affects both.
What Causes Aphasia and Apraxia?

Aphasia and apraxia of speech share most of their causes, since both stem from damage to the left hemisphere of the brain. What differs is which specific region sustains the injury. The five most common causes for adults are listed below.
Stroke
Stroke is the leading cause of both aphasia and apraxia in adults. When a clot blocks blood flow or a vessel ruptures in the left middle cerebral artery territory, the language network and the motor planning regions can both lose oxygen within minutes. Survivors often present with a mix of the two disorders, and our overview of stroke recovery speech therapy exercises covers the early rehabilitation period.

Speech Therapy for Stroke & Aphasia
Check this out for more information!
Traumatic Brain Injury
Traumatic brain injuries from falls, motor vehicle accidents, or assaults can damage the language and motor speech regions in patterns that vary widely. A diffuse injury tends to produce milder, mixed symptoms; a focal contusion to the left frontal lobe can produce dense aphasia or apraxia. Recovery depends heavily on injury location and severity, which our guide to TBI speech therapy walks through.
Brain Tumor
Tumors in or near the left hemisphere can produce slowly progressive aphasia or apraxia symptoms as they grow and compress surrounding tissue. Symptoms can also appear after surgery if the tumor sits in the eloquent cortex. The pattern depends on the tumor's location, size, and growth rate.
Neurodegenerative Disease
Some neurodegenerative conditions cause language and motor speech symptoms that resemble what stroke survivors experience, but progress over months or years rather than appearing suddenly. Primary progressive aphasia and the apraxic variant known as PPAOS are two recognized forms, and Alzheimer's disease and frontotemporal dementia can produce similar declines. Our resource on primary progressive aphasia covers one of these patterns.
Brain Infections
Encephalitis, meningitis, and brain abscess can damage left hemisphere tissue and produce aphasia, apraxia, or both, depending on which regions are involved. Recovery often tracks with how quickly the infection was identified and treated.
Types of Aphasia and Apraxia

Neither aphasia nor apraxia of speech is a single, uniform condition. Each has multiple subtypes that map to different patterns of brain damage and produce different symptoms.
Types of Aphasia
Aphasia subtypes are classified by which language abilities remain relatively intact and which are most disrupted. Some affect speech production primarily; others affect comprehension, and a few involve both.
Broca's aphasia. Also called non-fluent aphasia, this type causes slow, effortful speech with limited grammar but relatively intact comprehension. Adults with this subtype know what they want to say but produce short, halting phrases.
Wernicke's aphasia. Also called fluent aphasia, this type causes speech that flows easily but lacks meaning, often filled with invented or incorrect words. Comprehension is significantly impaired, and the person often does not realize their speech is hard to follow.
Global aphasia. The most severe form, global aphasia, affects both production and comprehension across all language modalities. Speech output is minimal, and understanding is significantly limited.
Anomic aphasia. Word retrieval is the primary target of this subtype. Adults can speak fluently and understand others, but they routinely cannot recall the specific word they need.
Conduction aphasia. Comprehension and production are relatively intact, but repeating words or phrases is unusually difficult. The disconnect points to damaged pathways between language regions.
Transcortical aphasia. A less common group of subtypes that includes the motor variant, which makes initiating speech difficult, and the sensory variant, which affects comprehension while preserving repetition.
Anomic aphasia is one of the more frequently encountered milder forms in clinical practice, and it often persists as a residual symptom after other aphasia features have improved.
Types of Apraxia
Apraxia of speech is generally divided into two categories based on when it appears in life.
Acquired apraxia of speech. Most common in adults, this form follows stroke, traumatic brain injury, brain tumor, or neurodegenerative disease. It can occur on its own or alongside aphasia, dysarthria, or both.
Childhood apraxia of speech. Present from early childhood, this developmental form is unrelated to stroke or brain injury. Genetic factors are believed to play a role, though the exact cause is not yet fully understood.
Acquired apraxia of speech can also appear alongside dysarthria, a separate motor speech disorder caused by muscle weakness rather than planning disruption.
How Aphasia and Apraxia Are Diagnosed

Diagnosis usually begins in the hospital after a stroke or injury and continues with a comprehensive evaluation by a speech-language pathologist. A neurologist is often involved as well, and our overview of neurological speech disorders in adults covers the broader diagnostic landscape. From there, the focus shifts to how these changes show up in real-life communication and what support is needed.
A strong evaluation looks at both test performance and everyday communication. Standardized testing is one piece of the puzzle, but it does not fully capture how someone functions in daily life. The goal is to connect clinical findings to what the person can actually do at home, at work, and in conversation.
The evaluation typically includes four components:
Language testing. Standardized assessments measure word retrieval, sentence comprehension, reading, writing, and the ability to follow multi-step directions. These results help identify patterns, but they are always interpreted in context, such as whether the person can keep up in conversation, express ideas clearly, or follow along in a group setting. The evaluation typically combines four components.
Motor speech assessment. The speech-language pathologist asks the adult to produce sounds, words, and phrases, watching for the inconsistent errors and effortful “groping” movements to distinguish apraxia from dysarthria or aphasia alone. These findings are tied back to real-life communication, such as difficulty getting words out smoothly, needing multiple attempts to say something, or avoiding speaking because it feels effortful.
Oral mechanism examination. The lips, tongue, jaw, and palate are checked for strength, range of motion, and coordination. Weakness points toward dysarthria; intact strength with disrupted coordination points toward apraxia.
Medical history and imaging review. MRI or CT findings, time since onset, and prior medical conditions all inform the diagnosis. The speech-language pathologist compares the imaging findings with observed communication patterns to gain a clearer sense of the overall picture.
Most importantly, real-life communication is assessed directly. The speech-language pathologist observes how the person communicates in conversation, how they handle breakdowns, and what support they need to get their message across.
When aphasia and apraxia co-occur, the speech-language pathologist documents the relative contribution of each. That distinction shapes the treatment plan and sets realistic expectations for progress.
How to Support Someone With Aphasia or Apraxia

Family members and close friends are often the most important communication partners for an adult living with aphasia or apraxia. Small adjustments to how you speak, listen, and structure conversations can dramatically reduce frustration on both sides.
Slow your pace and simplify your sentences. Short, direct sentences land more reliably than long ones, and pausing between ideas gives your loved one time to process. Avoid talking down or over-simplifying to the point of feeling patronizing.
Build in a wait time. Resist the instinct to fill silence or supply words. Allowing five to ten seconds of quiet often lets the person finish their thought on their own.
Use yes and no questions strategically. When word retrieval is hard, narrow choices help. Switch from open-ended questions to yes-or-no questions, and pair them with gestures or written cues when needed.
Honor the person's awareness. An adult with apraxia usually knows the word is wrong and is trying to fix it. Avoid finishing their sentences unless they specifically ask you to.
Ask the speech-language pathologist for guidance. Most speech-language pathologists offer conversation partner training, and a single session can transform daily communication at home.
Augmentative and alternative communication tools also play a meaningful role when speech output is significantly impaired. These range from picture boards and writing pads to speech-generating apps on a tablet, and the right tool depends on the adult's symptom profile and what feels natural in everyday use.
What We See Working With Clients

An adult who came to us six months after a left middle cerebral artery stroke arrived frustrated by family dinners. His family had been gently correcting his word-finding errors at the table, and he had begun pulling back from conversation altogether.
Most of the early work was with the family. Once they shifted from correcting to waiting, gave him space to land on the right word, and used yes-or-no questions when he stalled, his confidence at the table came back faster than his vocabulary did. He started initiating again within a few weeks.
Another client, recovering from a traumatic brain injury, had stopped leaving voicemails for his adult daughter. Anything longer than a short sentence collapsed into groping and inconsistent sounds, the classic pattern of apraxia of speech.
We layered in pacing boards and gradually increased phrase length, starting with two-word combinations and adding one word at a time. Within about eight weeks, he was leaving short voicemails again. His speech still required effort, but he had a tool that made longer messages possible.
Frequently Asked Questions About Aphasia and Apraxia

1. Can you have both aphasia and apraxia at the same time?
Yes, and it is actually common. The brain regions responsible for language processing and motor speech planning are located close together in the left hemisphere, so a single stroke or injury often damages both. A speech-language pathologist evaluates the contribution of each disorder and builds a treatment plan that addresses them in parallel.
2. Are aphasia and apraxia curable?
Neither condition is considered curable in the traditional sense, but both are treatable and can improve significantly with speech therapy. Many adults regain meaningful communication ability through consistent speech-language treatment, even years after the initial brain injury. How much progress is possible depends on the severity, the underlying cause, and how soon care begins.
3. What is Augmentative and Alternative Communication (AAC)?
Augmentative and Alternative Communication is a set of tools and methods that help adults express themselves when spoken language is limited. AAC ranges from low-tech options like picture boards, writing pads, and gestures to high-tech speech-generating apps on tablets or dedicated devices. A speech-language pathologist helps select and customize the right tool based on the adult's symptom profile and daily communication needs.
4. How do I know if my loved one has aphasia or apraxia?
The clearest signal is whether the breakdown is in finding and understanding words or in producing the sounds correctly. Aphasia tends to show up as trouble retrieving words, jumbled grammar, or difficulty following conversation, while apraxia shows up as inconsistent sound errors and visible struggle with mouth positioning. Only a speech-language pathologist can confirm which disorder is present, and adults frequently have both.
5. Can aphasia or apraxia be treated through online speech therapy?
Yes, online speech therapy works well for both conditions and is supported by a growing body of evidence. Video sessions allow the speech-language pathologist to clearly model mouth movements, share visual cues on screen, and involve family members in the same session from any location. Many adults find the consistency of weekly online sessions easier to maintain than driving to a clinic.
How Connected Speech Pathology Can Help

Our team of licensed speech-language pathologists specializes in adult speech therapy for neurological communication disorders, including aphasia and apraxia of speech. Every plan begins with a thorough evaluation that pinpoints the specific communication challenges and how they show up in daily life.
Sessions happen entirely online via secure video, removing the travel barrier and allowing family members to join from any location.
Speech therapy combines targeted approaches for language retrieval, motor speech sequencing, and conversation partner training, tailored to your loved one’s needs and adjusted to real-life situations as they progress. Schedule a free consultation to talk through what is going on and explore whether we are the right fit.
Summary
Aphasia and apraxia of speech are distinct conditions that can share similar causes and often occur together. Aphasia affects how the brain processes and organizes language, while apraxia affects how the brain plans and sequences the movements needed for speech.
Stroke is a common cause of both conditions in adults, typically involving areas of the left hemisphere that support language and speech. Because the symptoms can overlap, distinguishing between them requires a careful evaluation by a speech-language pathologist. That distinction helps determine what to target in therapy and how to prioritize treatment.
With consistent, targeted speech therapy and the support of trained communication partners, adults with either condition can make meaningful progress in their communication and participation in daily life.

About the Author
Allison Geller, M.A., CCC-SLP, is a communication coach, speech-language pathologist, and founder of Connected Speech Pathology, an international online practice providing professional communication coaching and speech therapy for children, teens, and adults. With more than two decades of experience, she has worked in medical and educational settings and published research on aphasia. Today, she leads a team of specialists who help clients improve their skills in public speaking, vocal presence, accent clarity, articulation, language, fluency, and interpersonal communication.