
Is a Lisp a Speech Impediment? Types, Impact, and When to Get Help

Is a lisp a speech impediment? Yes, a lisp is a common speech impediment, a functional speech disorder that changes how a person produces the /s/ and /z/ sounds. Here is what to know about a lisp: what kind of speech difference it is, the forms it takes, how it affects everyday communication, and when to seek help.
If you have a lisp or are a parent wondering whether your young child will outgrow one, this answer matters to you. Knowing whether a lisp is a true speech impediment or a normal part of speech development tells you if it needs speech therapy.
Most people picture a lisp as the "th" sound that replaces an /s/, but lisps take several forms and have different causes. Some fade as a child grows, and others stay without help.
Key Takeaways
A lisp is a functional speech disorder, a type of speech impediment that affects the /s/ and /z/ sounds. It is one of the most common speech sound differences in children.
There are four common types of lisps: interdental, dentalized, lateral, and palatal. Each one comes from a different tongue placement during speech.
Many children outgrow a lisp, but some need speech therapy. A frontal lisp can be typical before age four or five, while lateral and palatal lisps are not.
Speech therapy is an effective way to correct a lisp that lasts. A speech-language therapist helps children and adults reach proper tongue placement for clear speech.
Is a Lisp Considered a Speech Impediment?
How Speech Therapy Treats a Lisp
What We See Working with Clients
Is a Lisp Considered a Speech Impediment?

Yes, a lisp is a speech impediment. More precisely, a lisp is a functional speech disorder, which means it affects how clearly a person produces certain speech sounds without any damage to the brain or mouth. A lisp specifically changes the /s/ and /z/ sounds, the two that depend most on precise tongue placement.
About 23% of the clients a speech-language pathologist sees have a lisp, making it one of the most common conditions. Because a functional speech disorder arises from how a sound is produced rather than from a structural or neurological problem, it usually responds well to speech therapy.
The terms "speech impediment" and "speech disorder" refer to the same condition here. A lisp is also a type of articulation difference, since it affects how one or two specific sounds are formed rather than a child's whole system of speech.
A lisp is different from a language disorder. The words and grammar stay correct, and only the production of specific speech sounds is affected, so listeners often hear a "th" quality where an /s/ or /z/ should be.
A lisp also says nothing about a person's intelligence or effort. It is simply a learned pattern of placement, which is why so many articulate people have one and why it responds so well to practice.
Speech-language pathologists sort sound differences into articulation and phonological types, and a lisp is the articulation kind. The physical formation of the consonant sounds /s/ and /z/ is off, not the rules a child uses to organize speech.
To understand the basics of the sound itself, see our overview of what a lisp is.
Some lisps are part of normal speech development. When a young child pushes the tongue forward on /s/, they are often still learning the sound, while a lisp that lasts into later childhood or adulthood is treated as a speech impediment.
Types of Lisps
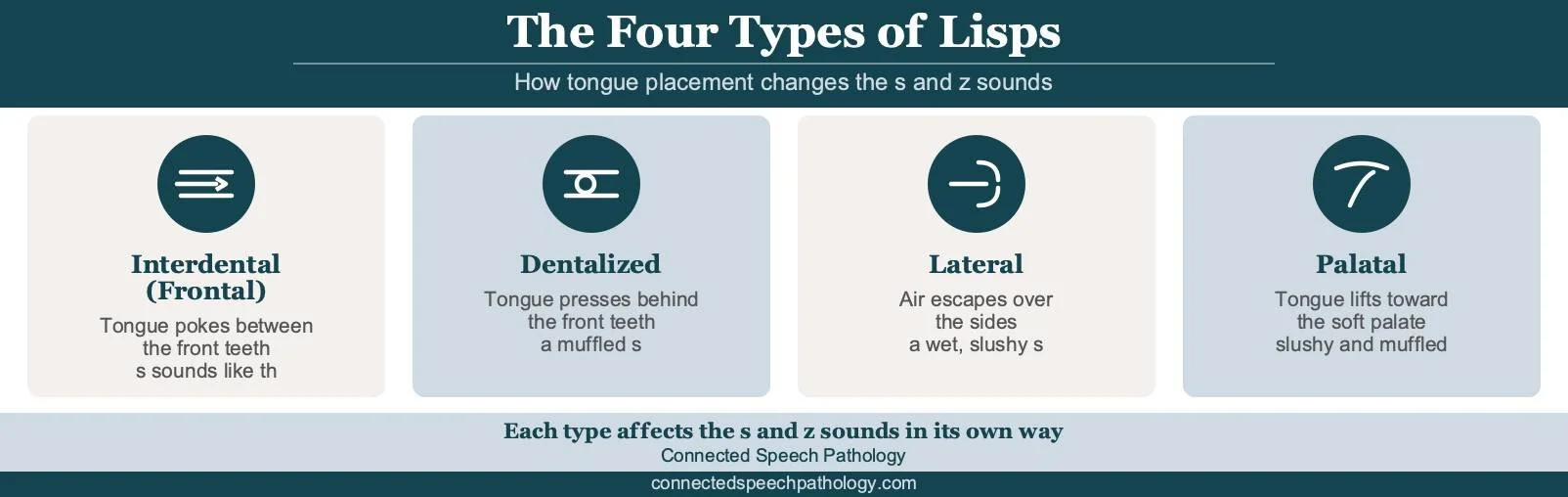
Lisps fall into four common types, and each one comes from a different position of the tongue during speech.
Interdental (frontal) lisp: an interdental lisp occurs when the tongue protrudes between the front teeth, so /s/ and /z/ sound like "th." This is the most familiar lisp and is common in young children.
Dentalized lisp: the tongue pushes against the back of the front teeth instead of slipping between them, which muffles the sound. It is also known as a dental lisp.
Lateral lisp: a lateral lisp occurs when air escapes over the sides of the tongue, giving /s/ and /z/ a wet or slushy quality, sometimes with excess saliva. A lateral lisp, sometimes called a lateralized lisp, is not part of typical speech development.
Palatal lisp: the tongue raises to touch the soft palate, the soft area toward the back of the roof of the mouth, which distorts the sound.
An interdental lisp and a dentalized lisp often resolve as a child's mouth and oral motor skills mature. A lateral lisp and a palatal lisp tend to persist and usually need speech therapy. A nasal lisp, where air escapes through the nose during these sounds, is less common.

Types of Lisps
Check out our blog discussing the types of lisps for more information!
How a Lisp Affects Daily Life

A lisp can affect more than the sound of a few words, since it can also shape how a person feels about speaking. The impact ranges from mild to significant, depending on the person and the setting.
A lisp can affect overall speech intelligibility, which is how easily a listener understands what is being said. When the /s/ and /z/ sounds are unclear, listeners may focus on the pronunciation rather than the message. Many people with a lisp report noticing this shift in listener attention more than the speech difference itself.
Everyday moments can bring the lisp into focus. Saying your own name, leaving a voicemail, ordering at a counter, or reading aloud in class all spotlight the /s/ and /z/ sounds, and difficult words can start to feel uncomfortable to say aloud.
Some people adapt by avoiding specific words containing /s/ and /z/, or by speaking less in group settings. Over time, this can affect speech clarity, communication skills, classroom participation, and confidence with public speaking.
Children rely on clear speech for academic success because so much early learning depends on reading aloud and being understood in class. A child with a lisp can also face teasing, which is one reason early support matters.
For adults, a lisp that has lasted for years can feel like a barrier at work, in interviews, or in social settings. Many adults start seeking speech therapy once a lisp begins to hold back how they want to show up.
None of this means a lisp must be fixed. Plenty of people speak with a lisp their whole lives and feel fine about it. The point is that help exists when a lisp gets in the way.
When to Seek Help for a Lisp

Seek help for a lisp if it lasts beyond the age when most children produce /s/ and /z/ clearly. Most children make these sounds correctly by about age five, so a lisp before then can simply be part of normal speech development.
Working with a speech therapist is recommended once a child is five years old or older and still has a noticeable lisp. A frontal lisp can be typical in toddlers, but a lateral lisp or a palatal lisp is not considered normal in children over four, and these types rarely go away on their own.
If a child's lisp persists after age seven, it is unlikely to resolve without speech therapy. There is room to wait and watch a young child's frontal lisp, but a lateral or palatal pattern is worth acting on early, since earlier help often means a shorter path to clear speech.
Parents are often the first to notice a lisp, and a pediatrician or teacher can flag it too. A referral is not required to book a speech evaluation, so families can reach out directly when something sounds off.
If you are unsure, an evaluation is a low-pressure way to get clarity. It is far easier to correct a lisp early than to undo years of practiced habit.
For parents weighing this decision, our parents' guide to speech therapy for kids walks through what to expect.
Adults can seek speech therapy, too. A lisp that continues into adulthood usually comes from habituated speech patterns, the motor habits the mouth has practiced for years, and these patterns respond well to focused, regular practice.
Our guide on what causes a lisp in adults explains why a lisp can develop or stay later in life, and why people have lisps covers the common causes in more depth.
What a Speech Evaluation Involves
A speech evaluation identifies the specific type of lisp and rules out any underlying structural or hearing-related cause. It is usually a single, low-pressure session that helps determine whether speech therapy is recommended and what treatment might involve.
The speech-language pathologist listens to the /s/ and /z/ sounds in isolation, in words, and during conversation, because a lisp can appear differently across speaking situations. They note whether the tongue moves between or behind the teeth, whether air escapes over the sides of the tongue, and how speech sounds during everyday communication.
The evaluation also includes a brief examination of the mouth and oral structures, along with a review of hearing history. Structural differences, tongue placement patterns, hearing difficulties, and other factors can all affect speech production, so these areas are considered early in the process.
Just as important, the speech-language pathologist asks how the lisp affects daily life. For a child, the concern may involve speech development, classroom participation, or confidence. For an adult, it may involve workplace communication, presentations, social situations, or a desire to speak more clearly and confidently.
Parents sometimes worry that the evaluation will feel like a test for their child. In practice, it usually looks like a combination of conversation, speech tasks, and age-appropriate activities. Adults typically experience the evaluation as a structured conversation about their speech, communication goals, and speaking situations that matter most to them.
At the end of the evaluation, clients leave with a clear understanding of the type of lisp, whether treatment is recommended, and what realistic progress may look like. That clarity is often a relief in itself.
How Speech Therapy Treats a Lisp

Speech therapy treats a lisp by improving the pronunciation of /s/ and /z/ sounds. The approach is practical and specific, and it works for both children and adults.
A speech-language pathologist first identifies the type of lisp and the factors contributing to it. Those factors may include speech habits, tongue placement patterns, hearing differences, oral structures, dental or jaw alignment, or other aspects of speech production.
From there, they build a treatment plan suited to the person's needs. Speech therapy often includes exercises for correct tongue placement, along with tactile cues that show exactly where the tongue should rest.
Most lisp treatment follows a clear path. The work starts with the sound on its own, moves to words, then to sentences, and finishes with everyday conversation, so the new habit holds up outside of sessions.
Progress depends on consistent practice. With regular speech therapy sessions and short practice at home between them, many people build the muscle memory for clear speech over a few months to a few years, depending on age and the type of lisp.
Home practice does not need to be long. A few minutes a day on the assigned sounds usually beats one long weekly drill, because a motor habit forms through frequent, short repetition.
Generalization is the last step. That is when the new /s/ shows up in real conversation without the person having to think about it. At that point, speech therapy can wind down.
For the specific techniques involved, see our guide on how to fix a lisp, and for the closely related "th" sound, our work on speech therapy for the th sound.
What We See Working with Clients

At Connected Speech Pathology, we work with children and adults whose lisps affect speech clarity, confidence, or day-to-day communication. The examples below reflect common situations we see in our work with children and adults who have lisps. Names and details have been changed to protect privacy.
One family contacted us about their six-year-old because teachers and relatives sometimes had trouble understanding him when he used words with /s/ and /z/ sounds. The lisp was becoming more noticeable as he spoke in longer sentences and participated more in school.
During speech therapy, we worked on accurate tongue placement and practiced the sounds in words, sentences, and conversation. Over time, his speech became easier for unfamiliar listeners to understand, and his parents noticed fewer requests for repetition.
Another client was an adult who had lived with a lateral lisp since childhood. He avoided speaking up during meetings, worried that coworkers would focus on how he sounded rather than on what he was saying.
Articulation therapy focused on improving sound production and carrying those skills into workplace conversations, presentations, and everyday communication. As his speech became clearer, he reported feeling more comfortable contributing ideas and participating in discussions without second-guessing himself.
The details vary from person to person, but the process is similar. We identify the situations that matter most, develop practical strategies, and build skills that carry over into everyday communication.
Frequently Asked Questions About Lisps

1. Is a lisp a speech impediment or a speech disorder?
It is both. A lisp is a speech impediment and, clinically, a type of functional speech disorder. The term describes a sound that is produced differently, not a problem with language or intelligence.
2. Can a lisp be corrected?
Yes, a lisp can be corrected with speech therapy. Many children outgrow a lisp on their own, and those who do not often respond well to speech therapy. Adults can correct a lisp with speech therapy, too.
3. What causes a lisp?
Lisps mostly occur due to incorrect tongue placement during speech. Habits like prolonged pacifier use, thumb sucking, or tongue thrust can play a role, and some lisps can be related to a tongue-tie. Mouth breathing and, rarely, a mild hearing loss can also affect how sounds develop.
4. At what age should I worry about my child's lisp?
Consider an evaluation if a lisp continues past age four. A toddler lisp is usually a frontal lisp and can be normal, but a lateral lisp and a palatal lisp are not. If it persists after age seven, it is unlikely to fade without help.
5. Can adults get rid of a lisp?
Yes, adults can work with a speech pathologist to improve their lisp. Speech therapy retrains tongue placement and builds new muscle memory for the /s/ and /z/ sounds. Consistent practice outside of treatment is beneficial.
6. Is a lisp the same as a speech delay?
No, a lisp and a speech delay are different. A lisp affects how a few specific sounds are made, while a speech delay means speech is developing later than expected overall. A child can have one, both, or neither.
How Connected Speech Pathology Can Help

Connected Speech Pathology provides online speech and language therapy for children, teenagers, and adults working on a lisp and other speech sound differences. Our speech-language pathologists assess each person's speech, develop a plan, and teach tongue placement to produce clear /s/ and /z/.
We offer speech therapy for adults and services for children, all delivered through live video sessions.
We also work with teenagers on speech sound goals, with a plan tailored to your age, your schedule, and the type of lisp you want to address.
Schedule a free consultation to see how clear, confident speech can feel.
Summary
So, is a lisp a speech impediment? Yes. A lisp is a speech impediment that affects the /s/ and /z/ sounds.
The four common types are interdental, dentalized, lateral, and palatal lisps. Each one is tied to a different tongue placement.
Not every lisp requires treatment, especially in very young children who are still developing speech sounds. The key question is whether the lisp is age-appropriate, improving over time, and affecting communication.
A lateral lisp, a palatal lisp, or any lisp that lasts past age seven usually needs speech therapy. A speech-language pathologist can help children and adults reach clear, confident speech.
Client Success Story: Real Results from Speech Therapy

About the Author
Allison Geller, M.A., CCC-SLP, is a communication coach, speech-language pathologist, and founder of Connected Speech Pathology, an international online practice providing professional communication coaching and speech therapy for children, teens, and adults. With more than two decades of experience, she has worked in medical and educational settings and published research on aphasia. Today, she leads a team of specialists who help clients improve their skills in public speaking, vocal presence, accent clarity, articulation, language, fluency, and interpersonal communication.