
How to Fix a Lisp at Any Age
A lisp is one of the most common speech impediments, affecting an estimated 23% of people who seek speech therapy. It occurs when the tongue is not positioned correctly during speech, distorting the /s/ and /z/ sounds, the two most frequently used consonant sounds in the English language. For children, teens, and adults alike, a lisp can affect clarity, confidence, and communication in daily life.
A lisp can be corrected at any age. Speech therapy for a lisp, also called articulation therapy, retrains the tongue to produce sounds correctly, and with consistent practice, most people make significant progress.
The sections below cover what causes a lisp, the four types of lisps, how speech therapy works, and what you can do at home to support your progress.
Key Takeaways
A lisp is a functional speech disorder caused by incorrect tongue placement during /s/ and /z/ production. It can persist into adolescence and adulthood without treatment.
There are four types of lisps: interdental (frontal), dentalized, lateral, and palatal. Each requires different treatment, and only the frontal and dentalized types resolve on their own in young children.
Speech therapy is the most effective treatment for a lisp at any age. Attempting to correct a lisp without professional guidance can reinforce the wrong muscle patterns and slow progress.
The sooner treatment begins, the faster the results, but adults and teens can achieve full correction with the right speech-language pathologist and consistent home practice.
How Do You Know If You or Your Child Has a Lisp?
How to Fix a Lisp with Speech Therapy
How Long Does It Take to Fix a Lisp?
Lisp Exercises to Practice at Home
What We See Working with Clients
What Is a Lisp?

A lisp is a functional speech disorder characterized by difficulty in producing the /s/ and /z/ sounds correctly. When these sounds are produced with the tongue in the wrong position, the airflow through the mouth is disrupted, creating the characteristic distortion listeners hear as a lisp.
The term "functional" means the root cause of the disorder is often unclear. There is no damage to the speech muscles or nervous system.
Lisps are classified as articulation disorders, a category of speech sound errors related to how specific sounds are physically produced. A speech-language pathologist (SLP) can identify the type of lisp, determine the contributing factors, and design a treatment plan to correct it.

What is a Lisp?
Interested in learning more about Lisps? Check out our blog!
What Causes a Lisp?

Lisps develop for a range of reasons. Most begin in early childhood, when a child is still developing speech patterns, and persist into the teen or adult years if left untreated. The most common causes of a lisp include tongue thrust, dental issues, anatomical differences, and learned speech habits.
Dental factors such as an overbite, open bite, or narrow dental arch can make it physically harder to produce a clean /s/ sound. An enlarged tongue, misaligned jaw, or tongue-tie (ankyloglossia) can have the same effect. When an anatomical issue is driving the lisp, a speech-language pathologist may recommend a consultation with a dentist or orthodontist in addition to speech therapy.
In many adults, a lisp is not caused by any structural issue. It's a residual habit from childhood.
The brain built a motor pattern for producing /s/ and /z/ sounds early on, and that pattern became deeply ingrained. Changing it requires systematic retraining, not just awareness.
Some people notice their lisp becomes more pronounced when they're tired, stressed, or speaking quickly. Motor patterns that aren't yet automatic break down under cognitive load, the same reason any new speech skill needs to be practiced until it becomes second nature.
Why Do People Have Lisps?
Tongue thrust: the tongue pushes forward or between the teeth during speech or swallowing
Dental alignment issues: overbite, open bite, or narrow dental arch
Anatomical differences: enlarged tongue or tonsils, jaw misalignment, or tongue-tie
Learned speech habits: incorrect tongue placement that developed in childhood and was never corrected
Prolonged pacifier use or thumb-sucking: these habits can affect tongue posture and dental structure during early development
For more details, see our guide on why people have lisps.
The Four Types of Lisps

Understanding which type of lisp is present is the first step in treatment. The four types each have distinct characteristics and different treatment approaches. A detailed overview is available in the types of lisps guide, and below is a clinical summary of each.
Interdental Lisp (Frontal Lisp)
An interdental lisp is the most common type. The tongue protrudes between the upper and lower front teeth during /s/ and /z/ production, so "sun" sounds like "thun" and "zero" sounds like "thero." This type is considered developmentally typical in children under 4.5 years old. A speech-language pathologist should evaluate it if it persists beyond age 6.
Dentalized Lisp
In a dentalized lisp, the tongue doesn't protrude outside the mouth but presses against the back of the front teeth instead of curling up toward the alveolar ridge. The resulting sound is muffled rather than sharp. Like the interdental lisp, the dentalized type can be a normal part of early speech development and often resolves by age 4.5.
Lateral Lisp
A lateral lisp occurs when air escapes over the sides of the tongue instead of flowing through the center of the mouth. The /s/ and /z/ sounds take on a wet, slushy quality.
One of the hallmark signs is that the person sounds like they have excess saliva in their mouth. Lateral lisps are not developmental; they don't resolve on their own and require speech therapy.
Palatal Lisp
A palatal lisp is the least common type. The middle part of the tongue contacts the hard or soft palate during /s/ and /z/ production, distorting the sound. Palatal lisps are not part of normal speech development and warrant evaluation as soon as they're identified.
Is a Lisp Ever Normal?

Interdental and dentalized lisps are considered developmentally typical in children under 4.5 years old. Young children are still developing the fine motor control needed to produce sibilant sounds, and mild frontal or dentalized /s/ errors are expected during this window.
Lateral and palatal lisps are never a normal part of speech development. Any child who displays one of these types should be evaluated by a speech-language pathologist regardless of age.
Children over 4.5- 6 years whose frontal or dentalized lisp has not resolved, and all teens and adults with any lisp type, benefit from speech therapy. A lisp does not go away on its own once these patterns are established.
How Do You Know If You or Your Child Has a Lisp?

The easiest way to check is to listen to the /s/ and /z/ sounds in everyday speech. Say the word "silly" aloud.
If the /s/ sounds like a "th," that's an interdental lisp. Say "zoo"; if it comes out as "thoo" or the /z/ sounds wet or slushy, those are lisp indicators.
You can also watch in a mirror. If the tongue tip is visible between the teeth when producing /s/ or /z/, that confirms an interdental lisp. A lateral lisp is harder to see but often audible: listen for a slushy or wet-sounding /s/ in words like "soda," "scissors," or "baseball."
Some people with a lisp also have difficulty with /sh/, /ch/, and /j/ sounds. If you're unsure whether a lisp is present, or which type, a formal evaluation with a speech-language pathologist is the clearest path to an answer. Connected Speech Pathology offers articulation therapy for adults and speech clarity therapy for children online.
How Is a Lisp Evaluated?

An evaluation by a speech-language pathologist is the starting point for treating a lisp. The goal is to determine which sounds are affected, what type of lisp is present, and whether any structural or motor factors are contributing.
A typical evaluation includes a review of the history of speech and language development, an oral-motor examination of the lips, tongue, jaw, teeth, and palate, and a formal articulation assessment. The SLP listens to how /s/ and /z/ are produced in single words, phrases, and connected speech, and conducts an interview to understand how the lisp is affecting daily communication and self-confidence.
For teens and adults, an evaluation often includes a conversational speech sample. Many people can produce a correct /s/ in isolation, but revert to their habitual pattern in natural speech. Knowing at which level the breakdown occurs shapes the treatment plan.
How to Fix a Lisp with Speech Therapy
Speech therapy for a lisp, also called articulation therapy, is the most effective treatment at any age. A speech-language pathologist does not simply tell someone where to put their tongue; they systematically build a new motor pattern through a structured hierarchy of practice.
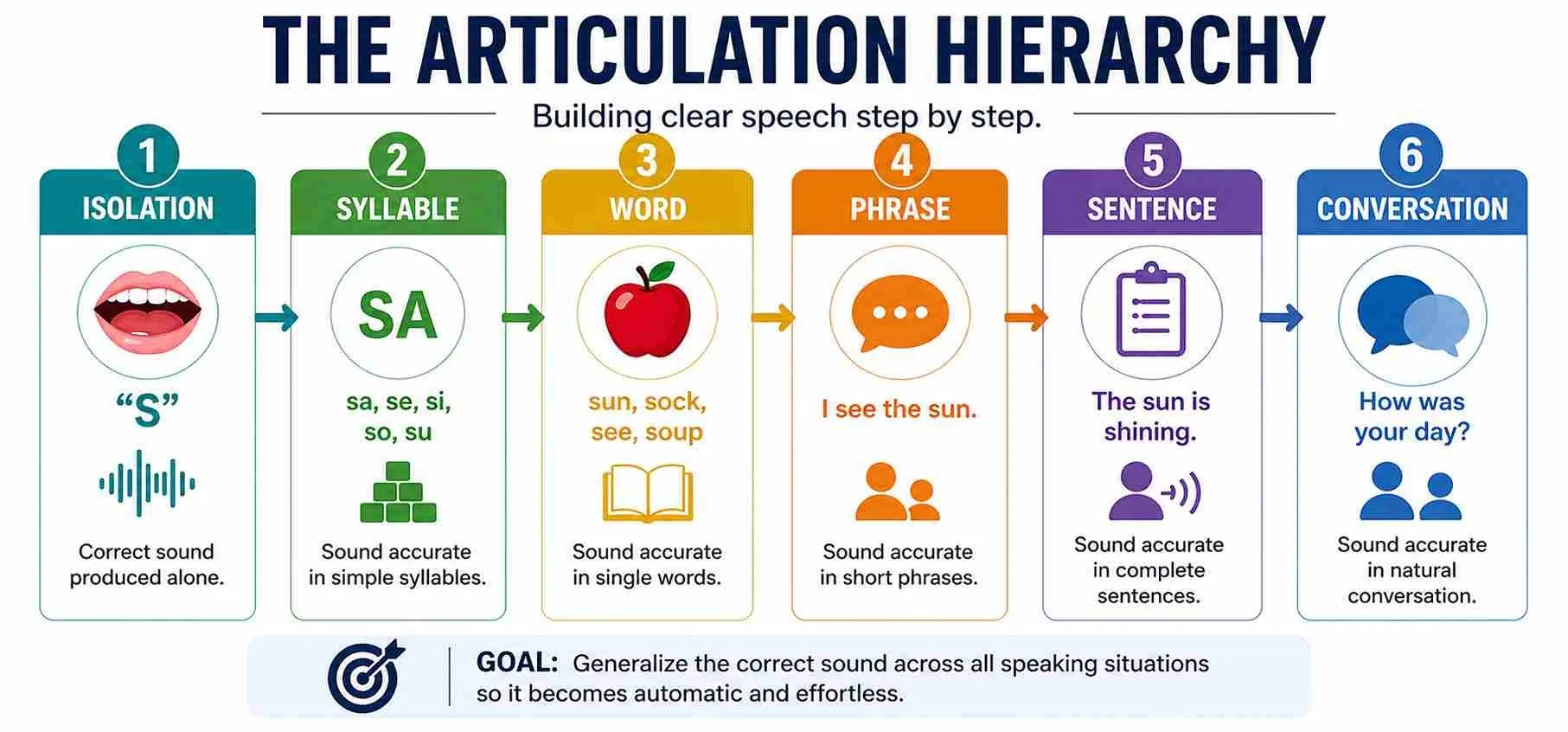
Speech treatment progresses through a series of steps: producing the correct /s/ sound in isolation, then in syllables, then in words, then in phrases and sentences, and finally in everyday conversation. Each level must be solid before advancing to the next. Jumping ahead before a new pattern is stable can solidify the wrong motor habit at a higher level, making correction harder.
Articulation therapy also includes oral-motor awareness training: learning to feel where the tongue should be, not just hear the difference. Visual feedback using a mirror is particularly useful for interdental lisps where the tongue position is visible. For lateral lisps, a speech-language pathologist uses specific tactile cues to help the individual find the correct central airflow pattern.
For children, speech therapy is structured as play-based activities and games to keep practice engaging. For teens and adults, sessions focus on awareness, targeted drills, and transfer to real-world communication contexts like presentations, meetings, and social conversations.
How Long Does It Take to Fix a Lisp?

The timeline for fixing a lisp depends on the type of lisp, the age at which treatment begins, the severity of the pattern, and how consistently home practice is maintained.
For young children with a frontal or dentalized lisp, treatment can take a few months of weekly sessions. For adults with a lateral lisp present since childhood, the process can take longer because deeply established motor patterns require more repetitions to override.
Adults and teens often move quickly through the early awareness stages because they understand the goal and can monitor their own output. The challenge is automaticity: producing the correct sound in conversation without having to think about it. Reaching that stage requires sustained, high-volume practice.
Speech therapy for a lisp is typically short-term compared to other communication interventions. Sessions are usually held once a week, lasting 30 to 45 minutes, with structured home practice in between. The more consistently someone practices between sessions, the faster progress tends to be.
Lisp Exercises to Practice at Home

Home practice is a core part of a lisp treatment. The exercises below support what a speech-language pathologist teaches in sessions. Always start home practice under the guidance of an SLP, because practicing the wrong pattern independently can make a lisp harder to correct.
These speech therapy tips for parents offer additional guidance for supporting a child at home.
Daily practice of 3 to 5 minutes is more effective than occasional longer sessions. Consistency builds the motor memory needed to transfer a new sound into automatic speech.
1. Mirror Practice
Stand in front of a mirror and smile with your teeth lightly together. Place the tongue tip just behind your upper front teeth, touching the alveolar ridge (the small bumpy ridge just behind your teeth). Slowly push air out over the tongue; the sound should be a smooth, continuous /ssss/ with no tongue visible between the teeth.
Practice this 10 times a day until the placement feels automatic.
2. The Exploding T Technique
Repeat the /t/ sound four times rapidly, then extend into a prolonged /sssss/: t-t-t-tsssss. The /t/ sound naturally positions the tongue just behind the upper teeth, making it a reliable springboard for /s/. Once this feels stable, practice words ending in /ts/: "mats," "pats," "hits."
3. Word-Level Practice
Once tongue placement feels consistent, practice /s/ and /z/ in words, starting at the beginning of words, then the middle, then the end. Choose one word position per day. Say each word slowly and deliberately, pausing to check tongue placement after each production.
4. Sentence Practice
Once the word level feels consistent, build target sounds into sentences. For children, making "silly sentences" with multiple /s/ words keeps practice engaging: "Sally saw six silly seals." For adults, read aloud from a book or article for two to five minutes daily, monitoring /s/ and /z/ sounds throughout.
5. Conversational Transfer
The final stage is the hardest: maintaining the correct pattern in natural conversation without monitoring every /s/ and /z/. Record yourself speaking for two minutes, then listen back and note how often the correct pattern holds. Tracking progress over weeks makes improvement visible and reinforces motivation.
What We See Working with Clients

For many of our adult clients, the biggest shift is not the sound itself. It's the moment they stop catching themselves.
Early in treatment, nearly every /s/ requires conscious effort, and conversations feel exhausting. By mid-treatment, the correct pattern starts to feel natural in low-pressure situations like reading aloud or one-on-one conversations.
Teens often show rapid progress once they understand the mechanics. Many arrive frustrated after years of being self-conscious about their speech in class presentations or social settings.
Once they can hear the difference and feel the correct placement, they tend to practice with high motivation. That consistency accelerates the timeline.
Children with lateral lisps typically need more time to establish a stable pattern than those with frontal lisps, but their improvement is often more dramatic. Parents frequently report that their child spontaneously begins monitoring their own speech outside of sessions, asking to practice more or correcting themselves mid-sentence. That's a reliable sign the new pattern is taking hold.
Client Success Story: Real Results from Speech Therapy
Frequently Asked Questions About Fixing a Lisp

1. Can adults fix a lisp, or is it too late for speech therapy?
Adults can fully correct a lisp at any age with speech therapy. Overriding an established motor pattern requires more repetitions than correcting a child's lisp, but the treatment approach is similar. Adult clients often move through the awareness stages quickly and see significant improvement within a few months of consistent practice.
2. What is the difference between a frontal lisp and a lateral lisp?
A frontal lisp (interdental lisp) occurs when the tongue protrudes between the teeth, replacing /s/ with a "th" sound. A lateral lisp occurs when air escapes over the sides of the tongue, producing a wet or slushy /s/. Frontal lisps are developmental and may resolve on their own in young children; lateral lisps don't self-correct and require speech therapy.
3. Should I wait to see if my child outgrows their lisp?
It depends on the type. Frontal and dentalized lisps are typically outgrown by age 4.5-5 years.
If your child is approaching five years old and the lisp persists, or if they have a lateral or palatal lisp at any age, an evaluation with a speech-language pathologist is recommended. Early intervention consistently produces faster results than delayed treatment.
4. Can a lisp affect a teenager's social life or academic performance?
Yes. Teens with a noticeable lisp often report feeling self-conscious during class presentations, social conversations, and other situations where they're speaking in front of others.
Speech therapy during the teen years is highly effective. Adolescents have the cognitive ability to understand and apply treatment techniques quickly, and motivation tends to be high because the social and academic stakes are clear.
5. Does online speech therapy work for a lisp?
Online speech therapy is highly effective for lisp treatment. A speech-language pathologist can use the camera to observe tongue placement and mouth position in real time, provide immediate feedback, and demonstrate correct placement up close. Many clients find online sessions more convenient and accessible, particularly for consistent weekly practice.
6. Is a lisp the same as a speech impediment?
A lisp is a type of articulation disorder that falls under the broader category of speech sound disorders. It affects the production of specific sounds (/s/ and /z/) rather than overall communication. With the right treatment, most lisps are fully correctable.
Is a Lisp a Speech Impediment? covers how lisps are clinically classified.
How Connected Speech Pathology Can Help

Connected Speech Pathology offers online speech therapy for adults, teens, and children with a lisp. Our speech-language pathologists specialize in articulation disorders and provide individualized treatment plans built around each client's lisp type, age, and communication goals.
Sessions take place online, which allows our speech therapists to use the camera to get close to the mouth for precise placement cues. This approach is just as effective as in-person therapy for articulation work.
Whether you're an adult who has never addressed a persistent lisp, a parent concerned about your child, or a teen preparing for a major presentation, our team is ready to help you speak with clarity and confidence.
Summary
A lisp is a functional speech disorder caused by incorrect tongue placement during /s/ and /z/ production, the two most common consonant sounds in English. The four types of lisps are interdental, dentalized, lateral, and palatal, each requiring a different treatment approach. Speech therapy for a lisp uses a structured articulation hierarchy, from isolated sound production up to conversational speech, to retrain the tongue and build automatic, accurate speech patterns.
Children, teens, and adults all benefit from treatment, and a lisp can be corrected at any age with consistent practice guided by a speech-language pathologist. Early intervention leads to faster results, but it is never too late to seek speech therapy for a lisp.

About the Author
Allison Geller, M.A., CCC-SLP, is a communication coach, speech-language pathologist, and founder of Connected Speech Pathology, an international online practice providing professional communication coaching and speech therapy for children, teens, and adults. With more than two decades of experience, she has worked in medical and educational settings and published research on aphasia. Today, she leads a team of specialists who help clients improve their skills in public speaking, vocal presence, accent clarity, articulation, language, fluency, and interpersonal communication.